Blood supply to the myocardium is derived from the two main coronary arteries, the left and the right (Fig. 16-11). These arteries originate from the aorta, immediately above the aortic valve. The left main coronary artery has two major branches known as the left anterior descending (LAD) and the left circumflex artery (LCA). The LAD passes down the anterior wall of the left ventricle toward the apex of the myocardium. The LAD supplies blood flow to the anterior two thirds of the ventricular septum, the anterior left ventricle, the apex, and most of the bundle branches (Table 16-2).
The LCA, the other branch of the left main coronary artery, sits in the groove between the left atrium and the left ventricle and wraps around the posterior wall of the heart. The LCA supplies blood flow to the left atrium, the lateral wall of the left ventricle, and the posterior wall of the left ventricle. In about 10% of the population, the LCA is the source of blood flow to the posterior descending coronary artery; when this pattern of flow occurs, the patient is referred to as left dominant. Branches of the LCA provide blood flow to the SA node in about 45% of people and to the AV node in about 10% of people.
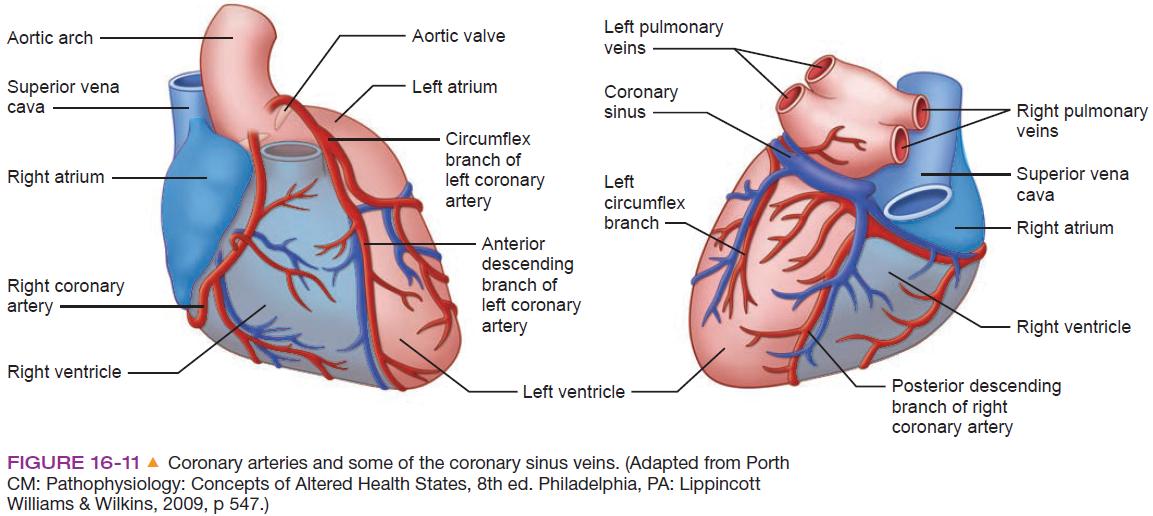
The right coronary artery (RCA) also comes off the aorta and branches toward the right atrium; the anterior, lateral, and posterior regions of the right ventricle; and the posterior
ventricular septum. The RCA provides blood flow to the right atrium, the right ventricle, and the inferior wall of the left ventricle. In about 90% of the population, the RCA is the source of blood flow to the posterior descending coronary artery, a pattern of flow known as right dominant. The RCA supplies oxygenated blood to the SA node in about 55% of people and to the AV node in about 90% of people.
The coronary arteries initially supply the epicardial layer of the heart and then pass deeper into the heart muscle to provide blood flow to the endocardium. As a result of this flow pattern, poor coronary blood flow initially deprives the subendocardial area of oxygenated blood. If the interruption to flow continues, the effects of decreased oxygenation expand throughout the thickness of the wall of the heart to the subepicardial surface.
Because the coronary arteries derive from the aorta (above the aortic valve) and lie between myocardial fibers, blood flow through the coronary arteries occurs when the aortic valve is closed during ventricular diastole, not systole. Therefore, anything that decreases the diastolic time (eg, tachycardia) decreases coronary perfusion.

Комментариев нет:
Отправить комментарий